

| Ward | Surgical ward | D.O.B/Age | 26 y.o |
| Consultant | Dr H. Vreede |
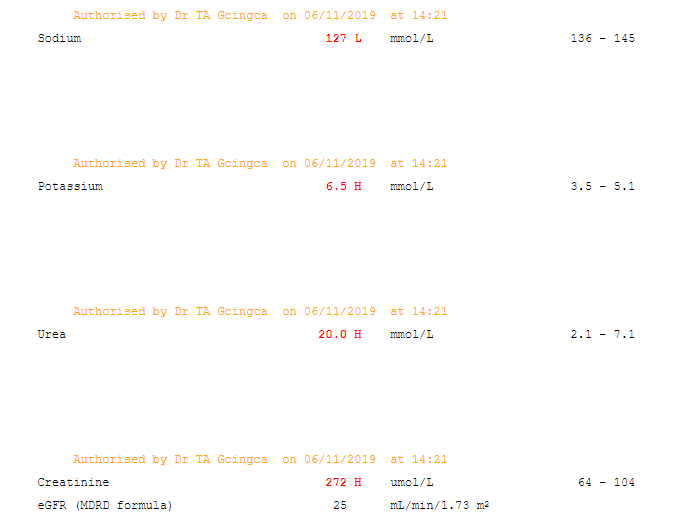
Abnormal result
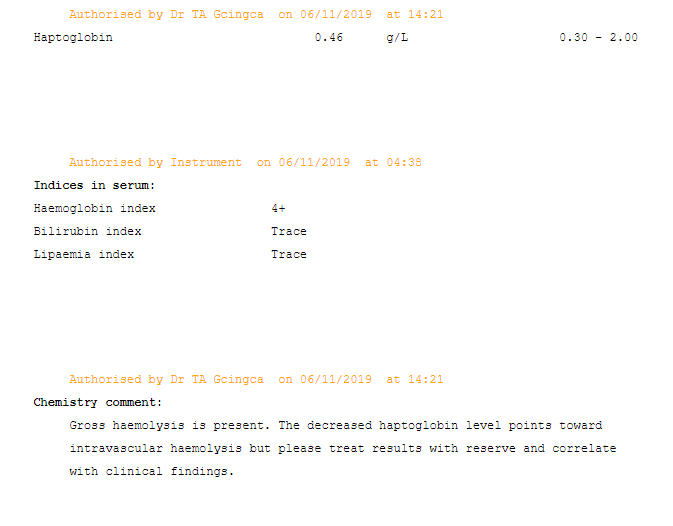
Indices in serum:
Haemoglobin index 4+
Bilirubin index Trace
Lipaemia index Trace
Presenting complaint
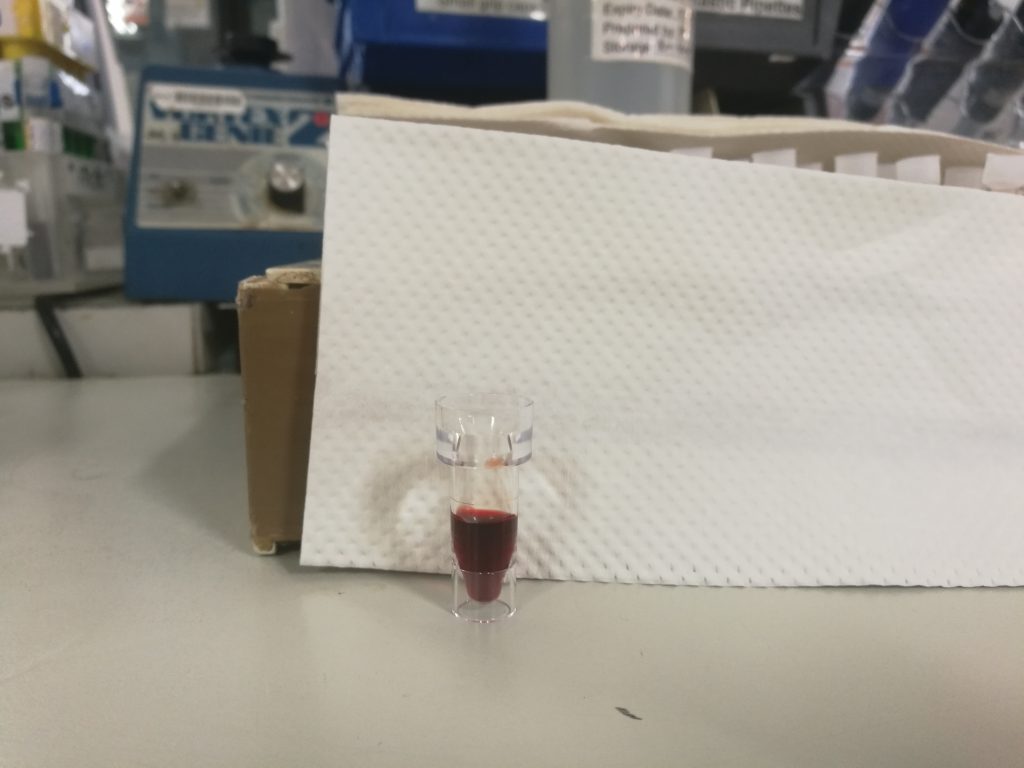
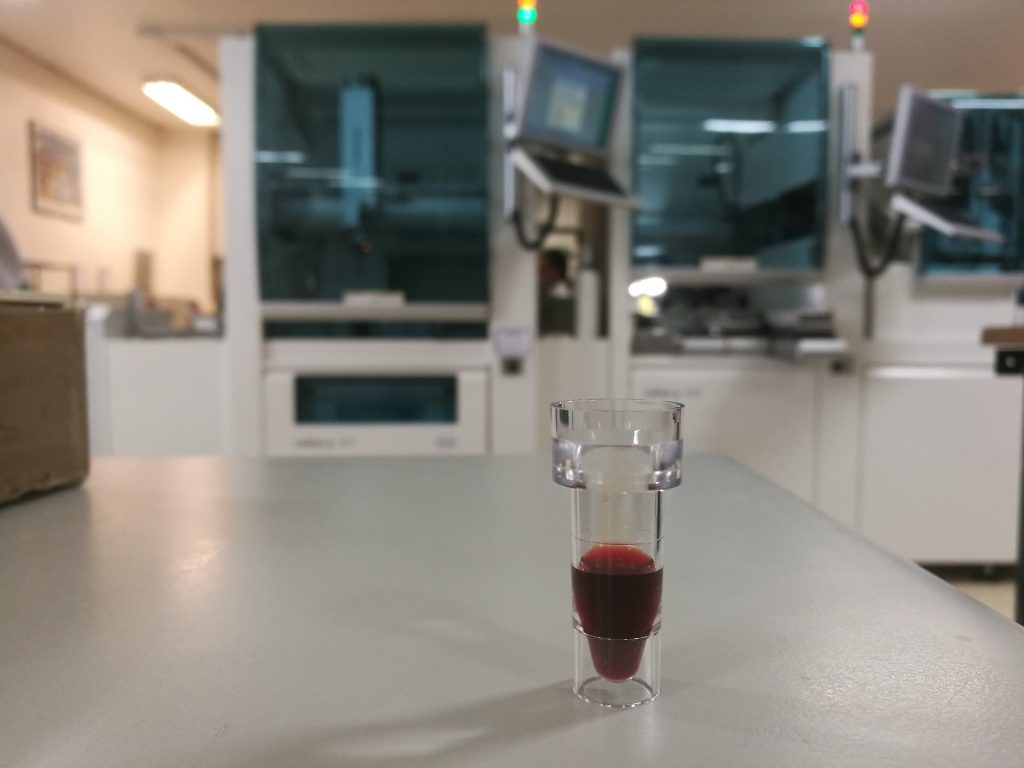
Call from a clinician to assist with generating results that were being rejected due to haemolysis.
History
26 y.o male
#Previously well
Admitted with multiple stab wounds and had a haemo-pneumothorax on the left side. Intercostal chest drain inserted. The patient acutely decompensated after 3 days being admitted. He was noted to have metabolic acidosis, hyperlactataemia, and symptoms of shock. The patient was not on any medication besides analgesia. No previous blood transfusion. No procedure in the ward.
Examination
Patient noted to be jaundiced. Urine coke-coloured. No petechiae. Patient not bleeding from any wound sites.
Laboratory investigations


Other investigations
CXR: haemopneumothorax on the left.
Final diagnosis
?sepsis ?toxin introduced through stab wounds
Take-home messages
Intravascular haemolysis results in the release of cell-free haemoglobin, red blood cell (RBC) stroma, and non-stroma proteins. Free haemoglobin binds nitric oxide (NO) at rate 1000 times that of RBC. Haemoglobin scavenging leads to decreased bioavailability of NO and thus vasoconstriction and alterations in capillary response to hypoxia. RBC stroma, which is the cytoskeletal framework supporting haemoglobin, can also contribute to DIC pathogenesis via activation of platelets and coagulation cascade. RBC stroma has also been shown to increase blood pressure and is toxic to the glomerulus and renal tubule and thus can cause acute renal failure. Ultimately, increased cytokines and hypotension stimulate a compensatory sympathetic nervous system response contributing to renal, splanchnic, and cutaneous vasoconstriction that, in combination with pathophysiology described above, leads to shock and circulatory collapse.
Marked increase of lactate dehydrogenase and haemosiderinuria are typical of intravascular haemolysis. Several haemolytic markers are available to guide the differential diagnosis and to monitor treatment of haemolytic conditions. They include increased reticulocytes (an indicator of marrow compensatory response) elevated lactate dehydrogenase, reduced haptoglobin, and unconjugated hyperbilirubinemia.
However, increased reticulocytes, lactate dehydrogenase, and bilirubin, as well as reduced haptoglobin, are observed in conditions other than haemolysis that may confound the clinical picture.
Haptoglobin is a positive acute-phase reactant. It is a protein that binds irreversibly to free (oxy)haemoglobin liberated into the plasma during intravascular haemolysis. The haptoglobin-haemoglobin complex is removed rapidly by the reticuloendothelial system to prevent loss of haemoglobin in urine. Low levels are a diagnostic indicator of intravascular haemolysis (but may be low in liver disease or with endogenous or exogenous oestrogen). Elevated levels are associated with acute phase response, nephrotic syndrome and with corticosteroids.
It is interesting to note in this patient that his result is in the lower level of normal, pointing towards the possibility that haptoglobin may be markedly decreased


{kind=link}
{kind=link}