

| Ward | Casualty Department | D.O.B/Age | 04/12/1940 |
| Consultant |
Abnormal result
Prostate-specific Ag (PSA) 949.50 H ug/L <4.00
Presenting complaint
Urinary retention.
History
Request form: Lower urinary tract symptoms and urinary retention.
Examination
| Important clinical findings to assess for include: General: Temporal wasting, signs of urinary incontinence (e.g. any leaking noted, need to wear sanitary products) Abdominal: Assess for masses, palpable bladder from retention P.R: Assess prostate for size, consistency, tenderness. CNS: Assess for any neurological fallout as prostatic metastasis tend to metastasize to the lower vertebrae. |
Laboratory investigations
Creatinine 83 umol/L 64 – 104
eGFR (MDRD formula) >60 mL/min/1.73 m2
White Cell Count 5.01 x 109/L 3.92 – 10.40
Red Cell Count 5.39 x 1012/L 4.50 – 5.50
Haemoglobin 15.5 g/dL 13.0 – 17.0
Haematocrit 0.485 L/L 0.400 – 0.500
MCV 90.0 fL 83.1 – 101.6
MCH 28.8 pg 27.8 – 34.8
MCHC 32.0 L g/dL 33.0 – 35.0
Red Cell Distribution Width 13.2 % 12.1 – 16.3
Platelet Count 226 x 109/L 171 – 388
PATHOLOGICAL DIAGNOSIS:
Prostate, biopsy: Adenocarcinoma.
Other investigations
Imaging studies may be necessary if there is a concern for metastasis and these will be guided by the clinical presentation e.g. CXR if metastasis to the lungs is suspected vs MRI if there is a concern of vertebral collapse.
Final diagnosis
Prostatic adenocarcinoma.
Take-home messages
- Prostate-specific antigen (PSA) is a protein produced by normal prostatic cells. The majority of PSA is produced by the glands in the transitional zone of the prostate (BPH). The peripheral zone, where 80% of prostate cancers originate, produces very little PSA.
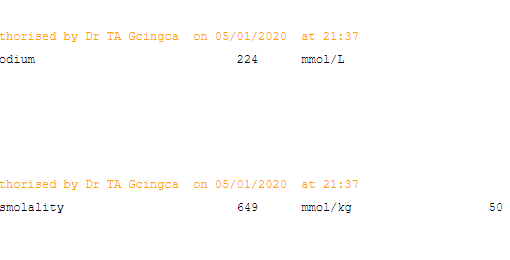
- An enlarged prostate can cause obstructive uropathy. The creatinine values in this patient do not suggest renal impairment though a baseline creatinine would be required to assess this.
- PSA is used for screening, diagnosis as well as monitoring of prostate related disease processes. PSA is an organ-specific, not a cancer-specific marker. It is useful in detection, staging and monitoring of prostate cancer.
- To improve diagnostic accuracy when PSA is between 4-10ug/L (“grey zone”), free PSA is measured and the free/total PSA ratio is calculated. Most normal PSA is protein-bound, and in prostatic cancer, a greater proportion is unbound. A free/total PSA ratio <0.25 increases the likelihood of cancer.

{kind=link}
{kind=link}