

| Ward | Medical ward | D.O.B/Age | 16/07/1950 |
| Consultant |
Abnormal result
Ammonia 251 H umol/L [11 – 35]
Presenting complaint
| Specimen request form has hepatic encephalopathy written as the diagnosis/reason for request. |
History
Unable to obtain.
Examination
Unable to obtain.
Laboratory investigations
| Sodium 143 mmol/L [136 – 145] Potassium 4.4 mmol/L [3.5 – 5.1] Urea 28.1 H mmol/L [2.1 – 7.1] Creatinine 359 H umol/L [64 – 104] eGFR (MDRD formula) 15 mL/min/1.73 m2 INR 2.77 Total bilirubin 54 H umol/L [5 – 21] Conjugated bilirubin (DBil) 36 H umol/L [0 – 3] Alanine transaminase (ALT) 34 U/L [10 – 40] Aspartate transaminase (AST) 113 H U/L [15 – 40] Alkaline phosphatase (ALP) 105 U/L [53 – 128] Gamma-glutamyl transferase (GGT) 33 U/L <68 |
Other investigations
| Unremarkable CMP. Elevated WCC of 11 otherwise normal FBC. Further investigations not requested on Trakcare. ?patient discharge vs transfer vs demise |
Final diagnosis
| ?Fulminant liver cirrhosis |
?End stage liver disease
Take-home messages
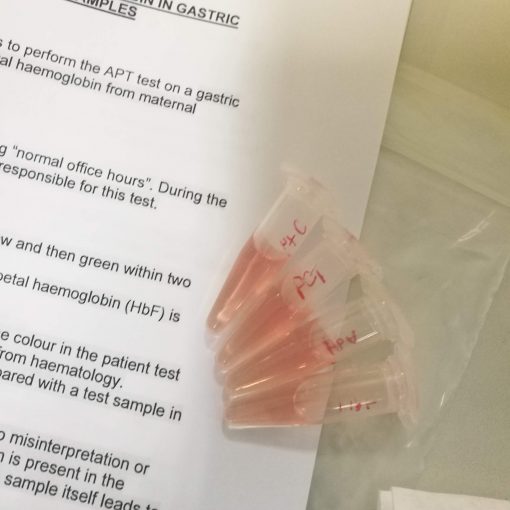
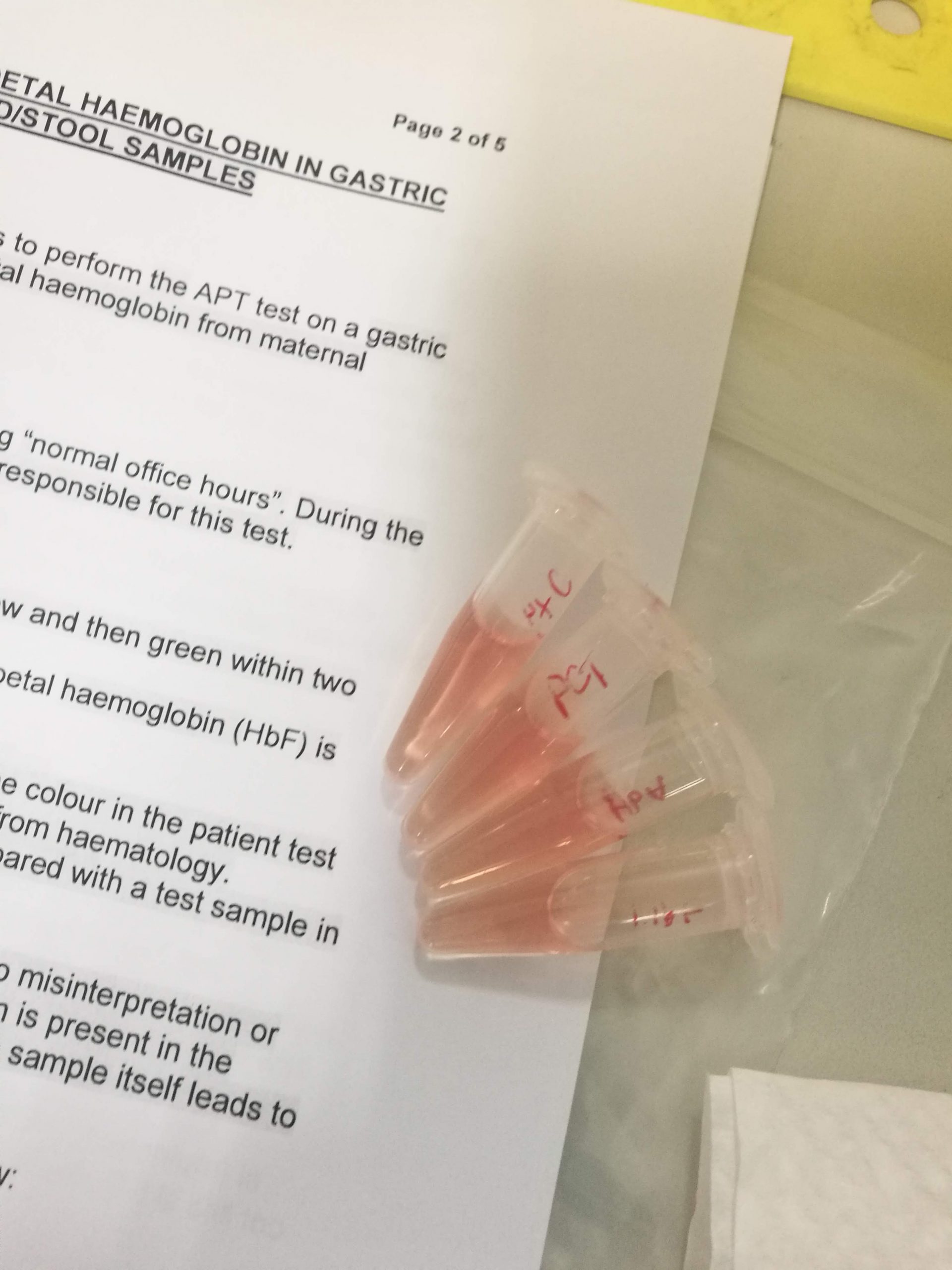
Most ammonia dealt with by the liver is produced by gut organisms. Protein degradation forms a smaller contribution. Ammonia in high concentrations is neurotoxic. It is detoxified by the liver to urea via means of the urea cycle, and urea is subsequently excreted in the urinePre-analytical factors including a delay in sample reception and sample not transported on ice may cause raised ammonia results.Other pre-analytical factors to consider include:
- No smoking by the person collecting the sample or the patient the sample is being collected from.
- Tourniquet should not be applied tightly or for too long (no tourniquet application ideal).
- Collected in an EDTA container.
- Must reach the lab within 15 to 20 minutes of being collected on ice.
- Patient should be fasted.
This patient has mildly deranged liver function tests and a prolonged INR suggesting liver disease which may be contributing to the hyperammonaemia. The unremarkable elevation in the liver enzymes may be due to a decrease of viable hepatocytes.


{kind=link}
{kind=link}
{kind=link}