

| Ward | Emergency unit | D.O.B/Age | 07/08/1968 |
| Consultant | Dr C. Hudson |
Presenting complaint
Request form: No clinical information provided
History
Unavailable.
Examination
Unavailable.
Laboratory investigations
Sodium 130 L mmol/L 136 – 145
Potassium 3.7 mmol/L 3.5 – 5.1
Urea 2.9 mmol/L 2.1 – 7.1
Creatinine 64 umol/L 49 – 90
eGFR (MDRD formula) >60 mL/min/1.73 m2
Glycated haemoglobin (HbA1c):
Glycated haemoglobin (NGSP) 6.5 %
Glycated haemoglobin (IFCC) 48 mmol/mol
Estimated average glucose (eAG) 7.8 mmol/L
Calcium 2.20 mmol/L 2.15 – 2.50
Total protein 86 H g/L 60 – 78
Albumin 28 L g/L 35 – 52
Total bilirubin 26 H umol/L 5 – 21
Conjugated bilirubin (DBil) 25 H umol/L 0 – 3
Alanine transaminase (ALT) 65 H U/L 7 – 35
Aspartate transaminase (AST) 444 H U/L 13 – 35
Alkaline phosphatase (ALP) 568 H U/L 42 – 98
Gamma-glutamyl transferase (GGT) 662 H U/L <40 Lipase 91 H U/L 13 – 60
Alpha-feto protein (AFP) 545010.0 H ug/L 0.0 – 7.0
Thyroid stimulating hormone 6.61 H mIU/L 0.27 – 4.20
Thyroxine (free T4) 13.7 pmol/L 12.0 – 22.0
White Cell Count 8.93 x 109/L 3.90 – 12.60
Red Cell Count 2.92 L x 1012/L 3.80 – 4.80
Haemoglobin 9.4 L g/dL 12.0 – 15.0
Haematocrit 0.278 L L/L 0.360 – 0.460
MCV 95.2 fL 78.9 – 98.5
MCH 32.2 pg 26.1 – 33.5
MCHC 33.8 g/dL 32.7 – 34.9
Red Cell Distribution Width 19.5 H % 12.4 – 17.3
Platelet Count 246 x 109/L 186 – 454

Other investigations
Abdominal ultrasound +/- CT scan may be helpful in detecting presence of liver mass +/- intra-abdominal masses.
Final diagnosis
?Hepatocellular carcinoma
Take-home messages
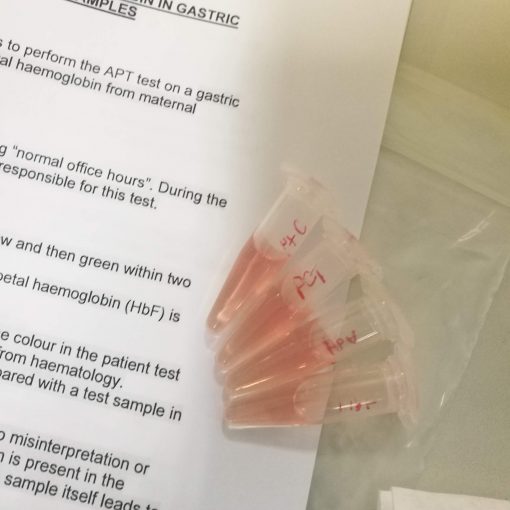
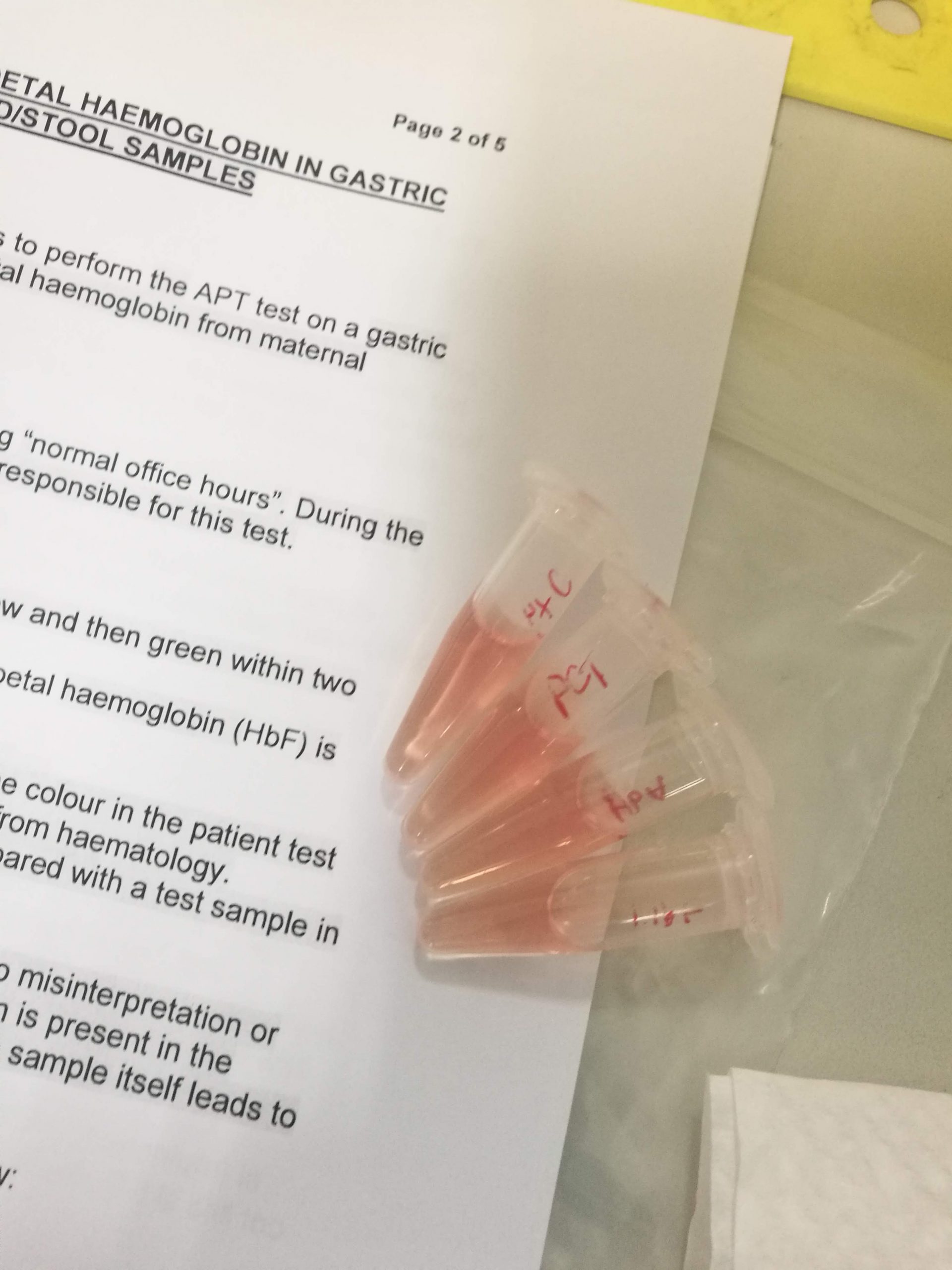
This case allowed me to become familiar with the concepts related to limitations of an assay. Having come across the need for dilution and the concept of high-dose hook effect, I found it interesting to see the gradual increase in AFP value as further dilutions were done. These are terms and concepts that this case allowed me to become familiar with.
Limit of Blank: This is the highest apparent analyte concentration expected to be found when replicates of a blank sample (containing no analyte) are tested. Detects “noise” that could interfere with the result.
Limit of Detection: This refers to the lowest analyte concentration likely to be reliably distinguished from the limit of blank and at which detection is feasible. LoD is determined using measured limit of blank, and test replicates known to contain a low concentration of an analyte.
Limit of Quantitation: This is the lowest concentration at which the analyte can not only be reliably detected but also at which some predefined goals for precision and bias are met. The LoQ may be equivalent to the LoD or it could be at a higher concentration. This is the limit that is clinically significant.

{kind=link}
{kind=link}
{kind=link}