

| Ward | Surgical OPD |
| D.O.B/Age | 03/06/1936 |
Abnormal result
Lipase 9640 U/L 13 – 60 (Result checked/analysed in dilution)
Hepatic enzymes suggestive of a mixed picture.
Presenting complaint
Request form: Jaundice ?NBL
History
Unable to obtain history. Questions to consider:
Presenting complaint: Weight loss, jaundice, yellowing of the sclera and/or skin, pruritis, vomiting, change in the colour of stool and/or urine, early satiety, epigastric fullness.
Past medical history: Any chronic illnesses e.g. diabetes, hypertension, epilepsy, HIV etc
Family history: especially GI malignancy.Social history: Diet, smoking, alcohol consumption, illicit drug use.
Examination
Vital signs: assess haemodynamic status
Gen: jaundice, scratch marks, any signs of wasting, mental status, pallor, oedema, clubbing, lymphadenopathy, fetor hepaticus
Abdo: signs of liver disease (spider naevi, caput medusa, ascites), hepatomegaly or cirrhosis, epigastric fullness, hepatic flap.
Full system examination of remaining systems.
Bedside tests: Glucose, urine dipstick, ABG
Laboratory investigations
Sodium 136 mmol/L [136 – 145]
Potassium 4.1 mmol/L [3.5 – 5.1]
Urea 7.2 mmol/L [2.1 – 7.1]
Creatinine 181 umol/L [49 – 90]
Total bilirubin 106 umol/L [5 – 21]
Conjugated bilirubin 87 umol/L [0 – 3]
Alanine transaminase (ALT) 200 U/L [7 – 35]
Aspartate transaminase (AST) 165 U/L [13 – 35]
Alkaline phosphatase (ALP) 365 U/L [42 – 98]
Gamma-glutamyl transferase (GGT) 519 U/L <40
Alpha-feto protein (AFP) 3.8 ug/L [0.0 – 7.0]
Carcinoembryonic Ag (CEA) 1.4 ug/L 0.0 – 5.0
CA 19-9 83 H kU/L 0 – 34
Other investigations
Urine dipstick: Unknown, but may be useful in assessing renal tubular integrity.
Final diagnosis
?pancreatic non-benign lesion
?gastric malignancy in pancreas
?gallstone pancreatitis
Take-home messages
- Most tumour markers are made by both normal cells and cancer cells, but they are made in larger amounts by cancer cells. A tumour marker may help to diagnose cancer, plan treatment, or find out how well treatment is working or for recurrence. It is recommended however that tumour markers should not be used for diagnosis but rather for monitoring of patients.
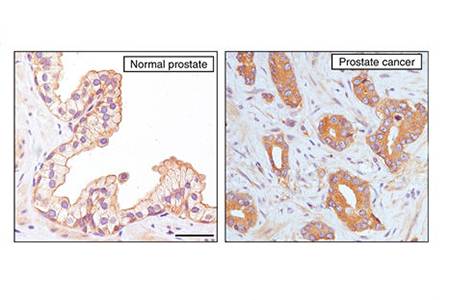
- Normally synthesised by human pancreatic and biliary duct cells, as well as gastric, colon, endometrial and salivary epithelia. As a tumour marker, it is used for adenocarcinoma of the pancreas (↑ in 80% of cases), but the rise is too late to be useful in early disease.
- High dose hook effect can affect immunoassays giving falsely lowered result. This can be overcome with dilution.


{kind=link}
{kind=link}
2 thoughts on “1. CA 19-9”
Glad to see you are using WordPress now Thando! 😉
Nice case!
It appears that the clinicians may have indeed used this test in this case as a screening test rather than a monitoring tool for disease progression, which is what we see quite often with these tumour markers. That is why we have the automatic canned comment on TrakCare which states what you said. Unfortunately clinicians often have no other thing to screen for a disease, and so tumour markers are then used for screening, as which is clear in what was on the request form in this case. Unfortunately it now appears to be acute pancreatitis, in which case the utility / meaning of the raised CA19-9 is uncertain, I would say.
Remember high dose hook-effect are more likely with sandwich immunoassays, as in this case.
Nice case for illustration!
Thanks Diets! It was a bit of a learning curve but I am absolutely loving it.
Thank you for your comment and I agree that most clinician’s seem to be aware that tumour markers should not be used for diagnosis. The difficulty comes in when modalities required for diagnosis (imaging studies, needing theatre time to do a biopsy, etc.) are limited or unavailable. At least having biochemical evidence of raised markers can help to narrow the list of differentials.